Frequently Asked Questions
For Professionals
The Hemobag®
The quickest, easiest, most efficient and risk free way to salvage precious autologous Whole Blood in cardiac surgery
Using the The Hemobag® saves whole blood not just red cells, and it takes less time to hemoconcentrate the same amount of blood than a cell washer could.
The Hemobag® and TS3 Tubing Set have been cleared by the FDA & CE for Clinical Use and are now available to purchase. To find out more about this Breakthrough Device that will change the way that Blood is Salvaged in Surgery, Contact Us.
The Hemobag® is capable of salvaging blood from any anticoagulated extracorporeal circuit in any area. As long as there is anticoagulated blood in a circuit circulated or collected and held outside the body for return to the patient, the Hemobag® will have an application for this blood.
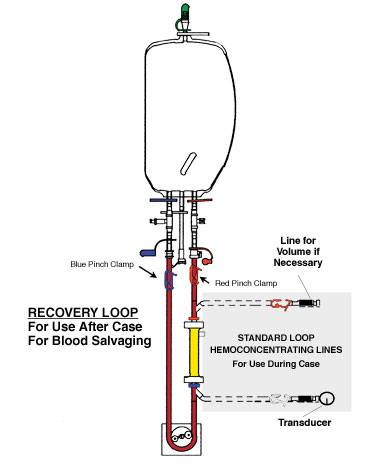
Yes. Before filling the Hemobag® in the field, a pressure tubing line can be filled to the inlet port and the patient by Anesthesia with a 3-way stopcock keeping a continuous loop.
The Hemobag® technology comes at a time when professionals everywhere are re-evaluating their views on blood management and transfusing patients and the consequences of doing so. If done correctly this technique recovers essentially all the patient's blood held in the CPB circuit. Using this technique saves whole blood not just red cells, and it takes less time to hemoconcentrate the same amount of blood than a cell washer could.
The Hemobag® can hold a maximum of 2.0 L.
Yes - The Hemobag® has a needleless sampling port for easy sampling at any time.
There are many variables such as hematocrit, flow rate, suction, siphon and type of hemoconcentrator used. It is important not to exceed the guidelines for the given hemoconcentrator used, but generally it takes about 8-10 minutes to do the whole process from start to finish.
No, the process is easy:
- Stop the pump and clamp the outlet port
- Start the pump again and allow crystalloid or air to chase the blood through the needless sample port of the circuit back to the Hemobag®
- Stop the pump just before the air or clear fluid enters the Hemobag®
- Disconnect, label and hand it to Anesthesia for reinfusion
No, it should not be pressurized, and as with all fluids for infusion, the Hemobag® must be completely de-aired and bubble-free before hanging for reinfusion by the large bore infusion port.
No. The Tubing Set for the Hemobag® works with any Hemoconcentrator with luer end caps and allows you to hemoconcentrate both during the case and after the case with the Hemobag® by way of its quick male and female quick connectors.
Yes, it is important to have the tubing set and hemoconcentrator primed and bubble-free prior to connecting the Hemobag® to reduce the blood to gas interface that stimulates the defences of blood and creates micro air.
Yes, the blood must be anticoagulated in order to process it through the hemoconcentrator and the Hemobag®. You will need to assess the need for additional protamine as per your hospital's protocol for the patient and give it separately to the patient after Hemobag® reinfusion. A Hepcon-type device would be useful in this situation. (Typical doses are between 10-50 mg.)
After filling the Hemobag® with the circuit's blood by crystalloid that has been chased through the circuit, the arterial and venous lines can be reconnected and recirculated like prebypass until the circuit is normally approved to be discontinued. You will now have time for other tasks such as hemoconcentrating the Hemobag®, which should only take about 8-10 minutes. You can then wait until the chest is closed and suck the circuit contents to a waste bucket or a cell washer, if you are still using one.
During the case the hemoconcentrator is used conventionally. After bypass any
¼ inch pump head not in use at the time can be used (e.g., sucker, vent, spare, empty).